From: WHO Media <Media@campaign.who.int>Date: February 12, 2024 at 5:20:15 AM EST
Subject: WHO Director-General's speech at the World Governments Summit – 12 February 2024
Monday, 12 February 2024
Your Highnesses, Your Excellencies,
Dear colleagues and friends,
Assalamu'alaikum warahmatullahi wabarakatuh.
I
thank Your Highnesses for your hospitality, for your steadfast support
for the World Health Organization and global health, and for the
opportunity to address you today.
It’s a great pleasure to be
back in Dubai. I was honoured to be here in December last year for COP28
– the first COP to include a day dedicated to health, and I thank the
UAE for its leadership in giving health such a prominent place in the
climate agenda. It was the first of its kind. Thank you, UAE, for being a
pathfinder.
147 countries signed the COP28 UAE Declaration on Climate and Health, recognising that the climate crisis is a health crisis.
In
particular, I thank the UAE for its support for the WHO Global
Logistics Hub here in Dubai, which has become an essential part of WHO’s
operational response to health emergencies around the world.
Last
year, the hub distributed medical supplies for 50 million people in
emergency situations in 81 countries, in every region of the world –
Afghanistan, Chad, Fiji, Haiti, Papua New Guinea, Sri Lanka, Ukraine,
Venezuela, Yemen and more.
Since the hub opened in 2015 in Dubai, it has expanded 7-fold, from 3000 to 20 000 square metres.
Indeed,
the hub is currently playing a vital role in our response to several
emergencies around the world, including the ongoing crisis in Gaza.
So
far, we have delivered 447 metric tons of medical supplies to Gaza, but
it’s a drop in the ocean of need, which continues to grow every day.
Only 15 out of 36 hospitals are still partially or minimally functional in Gaza.
Health workers are doing their best in impossible circumstances.
I
am especially concerned by the recent attacks on Rafah, where the
majority of Gaza’s population has fled from the destruction to the
north.
WHO continues to call for safe access for humanitarian personnel and supplies;
We continue to call for hostages held by Hamas to be released;
And we continue to call for a ceasefire.
===
Excellencies,
On the 12th of
February 2018 – exactly six years ago – I stood on this stage and said
the world was not prepared for a pandemic, and expressed my concern at
that time that a pandemic could happen anytime.
As you
remember, less than two years later, in December 2019, the COVID-19
pandemic struck, and indeed, the world was not prepared.
Today I stand before you, in the aftermath of COVID-19,
With millions of people dead,
With social, economic and political shocks that reverberate to this day,
Although
some progress has been made, like improvements in surveillance, the
Pandemic Fund, building capacities in vaccine production and the
periodic review we have started, still, the world is not prepared for a
pandemic.
The cycle of panic and neglect is beginning to repeat. [Really?
Let's see if the US stopped spending on pandemics and biodefense
between outbreaks. Hmm, it actually spent about 11 $Billion/year year
in, year out, regardless of outbreaks. And Europe is spending a ton to
beef up its biosecurity systems despite the absence of any pandemic.
Where does Tedros get his “facts” from?—Nass]
The
painful lessons we learned are in danger of being forgotten as
attention turns to the many other crises confronting our world.
But if we fail to learn those lessons, we will pay dearly next time. [Scaremongering.]
And there will be a next time. History teaches us that the next pandemic is a matter of when, not if. [History
teaches there was only one significant pandemic in the 20th century.
But in the 6 years that Tedros has been the D-G of the WHO, he declared
3!]
It may be caused by an influenza virus, or a new
coronavirus, or it may be caused by a new pathogen we don’t even know
about yet – what we call Disease X.
There’s been a lot of attention on Disease X recently, but in fact, it’s not a new thing. [Nor is it a real thing.]
We
first used the term Disease X in 2018 – the same time as I spoke here
at this World Governments Summit – as a placeholder for a disease we
don’t even know about yet, but for which we can nonetheless prepare.
COVID-19 was a Disease X – a new pathogen causing a new disease.
But there will be another Disease X, or a Disease Y or a Disease Z.
And as things stand, the world remains unprepared for the next Disease X, and the next pandemic.
If it struck tomorrow, we would face many of the same problems we faced with COVID-19. [Funny how he NEVER tells us what those problems are and how his program will solve them…]
It’s
for this reason that in December 2021, WHO’s Member States met in
Geneva and agreed to develop an international agreement on pandemic
preparedness and response – a legally-binding pact to work together to keep themselves and each other safe. [Need I say more?—Legally binding and WHO/Tedros gives the orders.]
Countries
set themselves a deadline to complete the agreement in time for
adoption at the World Health Assembly in May of this year.
That’s now just 15 weeks away.
However, there are currently two major obstacles to meeting that deadline.
The first is a group of issues on which countries have not yet reached consensus.
They’re making progress, but there are still areas of difference that need further negotiation between countries.
None
of them are insurmountable. If countries listen to each other’s
concerns, I am confident they can find common ground and a common
approach.
The second major barrier is the litany of lies and conspiracy theories about the agreement:
That it’s a power grab by the World Health Organization;
That it will cede sovereignty to WHO;
That it will give WHO power to impose lockdowns or vaccine mandates on countries;
That it’s an “attack on freedom”;
That WHO will not allow people to travel;
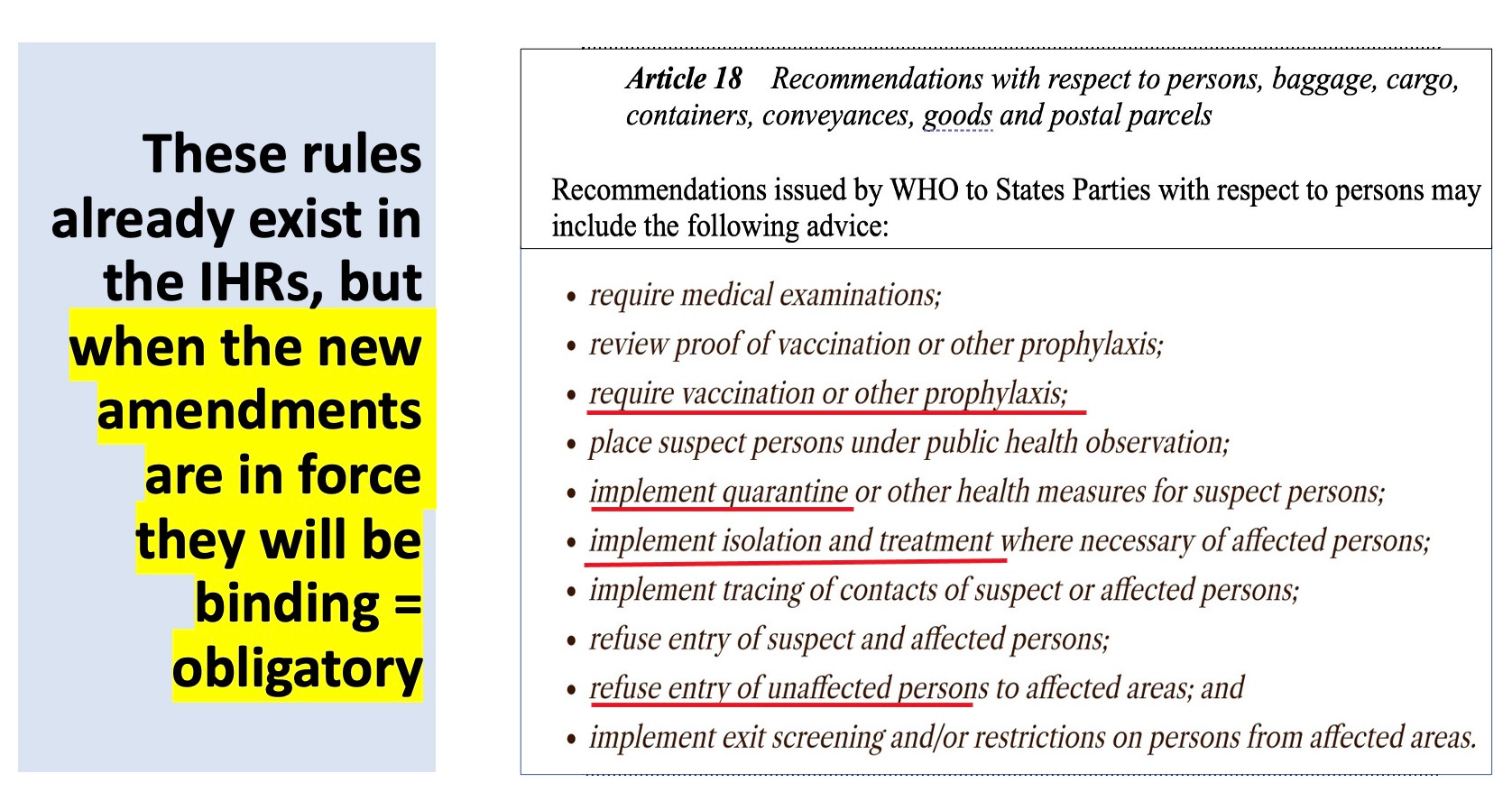
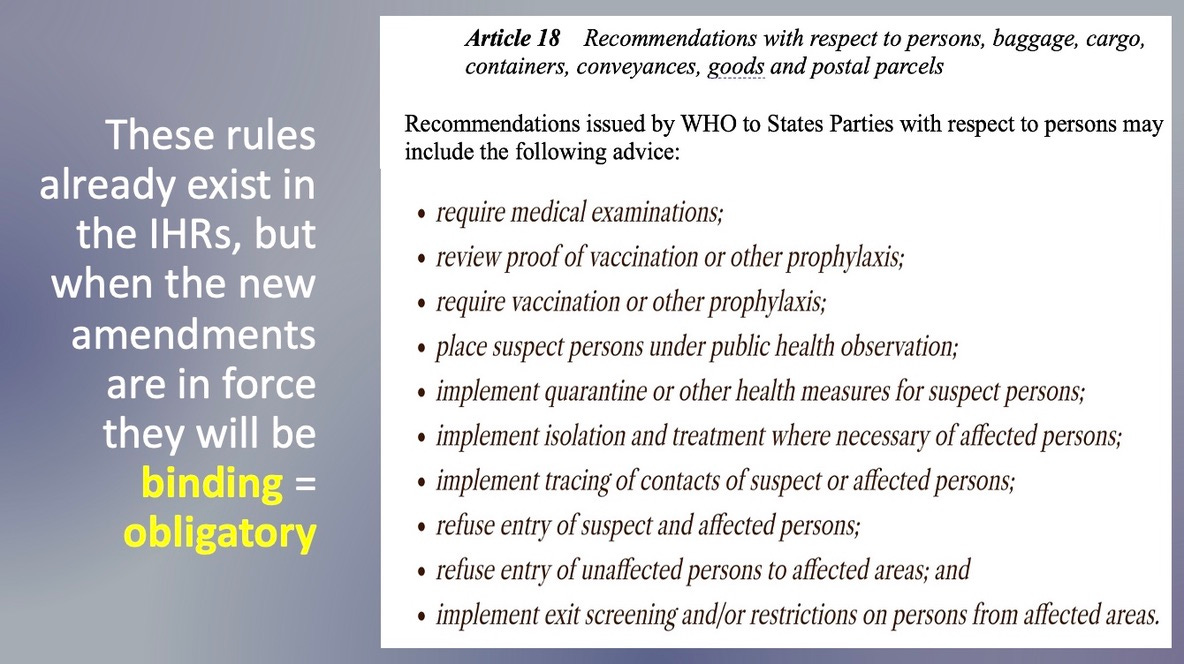
And that WHO wants to control people’s lives. (Below
is a screenshot of Article 18 of the current IHR—the recommendations
listed become binding orders if the Amendments are adopted. Tedros lies
by claiming the “agreement” does not include these orders. But they
are located in the Amendments and they definitely would give WHO all
these powers)
These are some of the lies that are being spread.
If they weren’t so dangerous, these lies would be funny.
But they put the health of the world’s people at risk. And that is no laughing matter. [What a sick joke.]
These
claims are utterly, completely, categorically false. The pandemic
agreement will not give WHO any power over any state or any individual,
for that matter.
Anyone who says it will is either uninformed or lying.
But don’t take my word for it. The draft agreement is available on the WHO website for anyone who wants to read it. [Notice how he makes sure not to include the URL. So I will. https://apps.who.int/gb/inb/pdf_files/inb7/A_INB7_3-en.pdf ]
And anyone who does will not find a single sentence or a single word giving WHO any power over sovereign states. [Read my last substack post and laugh your *** off.]
You
know, countries are even talking about sovereign AI, as we have seen in
the previous panel, in the same way. Countries will keep their
sovereignty.
That’s because it’s sovereign states themselves who are writing the agreement. Why would they agree to cede sovereignty to WHO? [Good
question, and the answer is because many countries are controlled by
the same power that is controlling Tedros and the WHO. You didn’t
really think Biden or Trudeau or Rishy Sunak were “running” their
countries, did you?]
We cannot allow this historic agreement, this milestone in global health, to be sabotaged by those who spread lies, either deliberately or unknowingly. [He meant headstone, the stone that sits on your grave. Or maybe he meant Blackstone.]
Let
me be clear: WHO did not impose anything on anyone during the COVID-19
pandemic. Not lockdowns, not mask mandates, not vaccine mandates.
We don’t have the power to do that, we don’t want it, and we’re not trying to get it. [Pardon me, has Tedros read the treaty and amendments?]
Our
job is to support governments with evidence-based guidance, advice and,
when needed, supplies, to help them protect their people. [This
is what the WHO has historically done, but if the treaty and amendments
go through, they transform the WHO so that it will govern health,
globally.]
But the decisions are theirs. And so is the pandemic agreement.
It
has been written by countries, for countries, and will be implemented
in countries in accordance with their own national laws. [Then why was the last draft of the treaty named the “Bureau Text” when Bureau referred to the WHO bureaucracy? Why does the BMGF
have a seat at the negotiating table if the treaty cum agreement is
only being written by countries? Why does the treaty draft require
nations to pass laws they may not want, such as providing liability
protection to the makers and distributors (including the WHO) of
untested pandemic vaccines?]
In fact, WHO will not even be a party to the agreement. The parties are governments and governments alone. [Is this a joke? How can you not be a party when you get to give all the orders?]
Far
from ceding sovereignty, the agreement actually affirms national
sovereignty and national responsibility in its foundational principles. [Now
you see why he didn’t provide the URL for the treaty or amendments.
Well, here is the place to read the amendments, color-coded for ease of
distinguishing what is being added: https://worldcouncilforhealth.org/wp-content/uploads/2023/05/WGIHR_Redlined-words-of-Proposed-Amendement-Compilation-en.pdf]
Indeed, the agreement is itself an exercise of sovereignty. [Spare me this confabulation.]
It’s about the commitments countries are making to keep themselves and each other safer from pandemics.
And it recognizes that they can only do that by working with each other. [The One Health approach.
Doctors are no longer able to take care of patients by
themselves—unless they are in a committee with veterinarians, plant
pathologists, climatologists and ecologists and they diagnose and treat
by majority vote there will be no medical care.]
Let
me tell you what the agreement does say. It’s a set of commitments by
countries to strengthen the world’s defences in several areas:
To strengthen prevention with a One Health approach;
The health and care workforce;
Research and development;
Access to vaccines and other products;
Sharing of information, technology, and biological samples;
And more.
Now I ask you: what is so problematic about those commitments?
Is there anyone who thinks countries should not cooperate?
Does anyone think countries should not share information? [Why should Guinea-Bissau have my medical records?]
Does anyone think some people are more deserving than others of access to vaccines and other tools? [Actually,
your own amendments say that some people get treated first. Perhaps
you should read the proposed IHR Article 2, which says that equitable
access to treatments can be ignored when necessary.]
In our interconnected and interdependent world, countries can only keep themselves safe if they work with each other. [This was never true in the past—it is just a specious claim to support your globalist agenda.]
In that sense, the pandemic agreement is a commitment to national security. It’s in every country’s own national interest.
Because
pathogens have no regard for the lines humans draw on maps, nor for the
colour of our politics, the size of our economies or the strength of
our military.
For everything that makes us different, we are one humanity, the same species, sharing the same DNA and the same planet.
We have no future but a common future. [Did I just see a Freudian slip?]
Common threats, then, demand a common response. [Agree, and that response should be: Get Stuffed!]
That’s why this pandemic agreement is so important.
===
Your Highnesses, Your Excellencies,
The COVID-19 pandemic inflicted huge losses on communities, countries, businesses and economies.
Those losses must not be in vain, and must not be repeated. [I
remember this argument from the Vietnam war: all those poor boys must
not have died in vain, so we have to keep fighting and more boys dying.
DUH?]
It’s possible, or even likely, that we will face another pandemic in our lifetimes.
We can’t know how mild or severe it might be. But we can be ready.
Are we ready now? Not yet.
That’s why the pandemic agreement is mission-critical for humanity.
It’s a pact with the future, that we will not expose the generations who follow us to the same suffering that we endured. [No, their suffering will be multiplied—as slaves—if your lot gets its way. I don’t think we are going to let that happen.]
Had the agreement been in place before COVID-19, we would not have lost so much.
Now
is the moment for leadership from the highest levels of government to
deliver the pandemic agreement to the World Health Assembly in 15 weeks’
time.
Now is the time to say no to inequity;
No to lies and misinformation;
And yes to international cooperation;
Yes to equity;
And yes to solidarity.
[How does this guy sleep at night pushing out all these lies and
misdirection to effect a complete globalist takeover of the world’s
resources and people?]
As the generation that lived
through COVID-19, we have a collective responsibility to protect future
generations from the suffering we endured. [The emotional blackmail doesn’t cut it any more. Getting jabbed with poison to save grandma only works once.]
May history record that we rose to that responsibility, and made the world a healthier, safer and fairer place.
Shukran jazeelan. I thank you.